When a medical person told me recently You can do without the PET scan ↗ you have had recommended, because we limit the number of scans people have so we don’t cause more problems than we find, it seemed a bit strange. I am in the fortunate position of working at a university where I have access to people who understand these things. So I made enquiries and learned that this was radiophobia, and it can cause people to miss out on healthcare. But I still wasn’t offered a scan.
In my case, something changed and out of the blue the NHS Scotland offered me a PET scan after all. I was happy, and when the friendly voice on the phone reassured me you will be a little radioactive after the scan… I responded sure, like living in Aberdeen makes me radioactive! because now I knew that was the comparison. They laughed in understanding, and that was that.
But later I received an official pre-scan booklet from NHS Scotland containing scary advice such as:
During the 4 hours after your scan you will need to follow these precautions:
• Avoid close contact with other people, such as hugging
• Avoid any contact with children or pregnant people - being at a distance of more than 1m away is fine.
After 4 hours has passed, you may return to all normal activities.
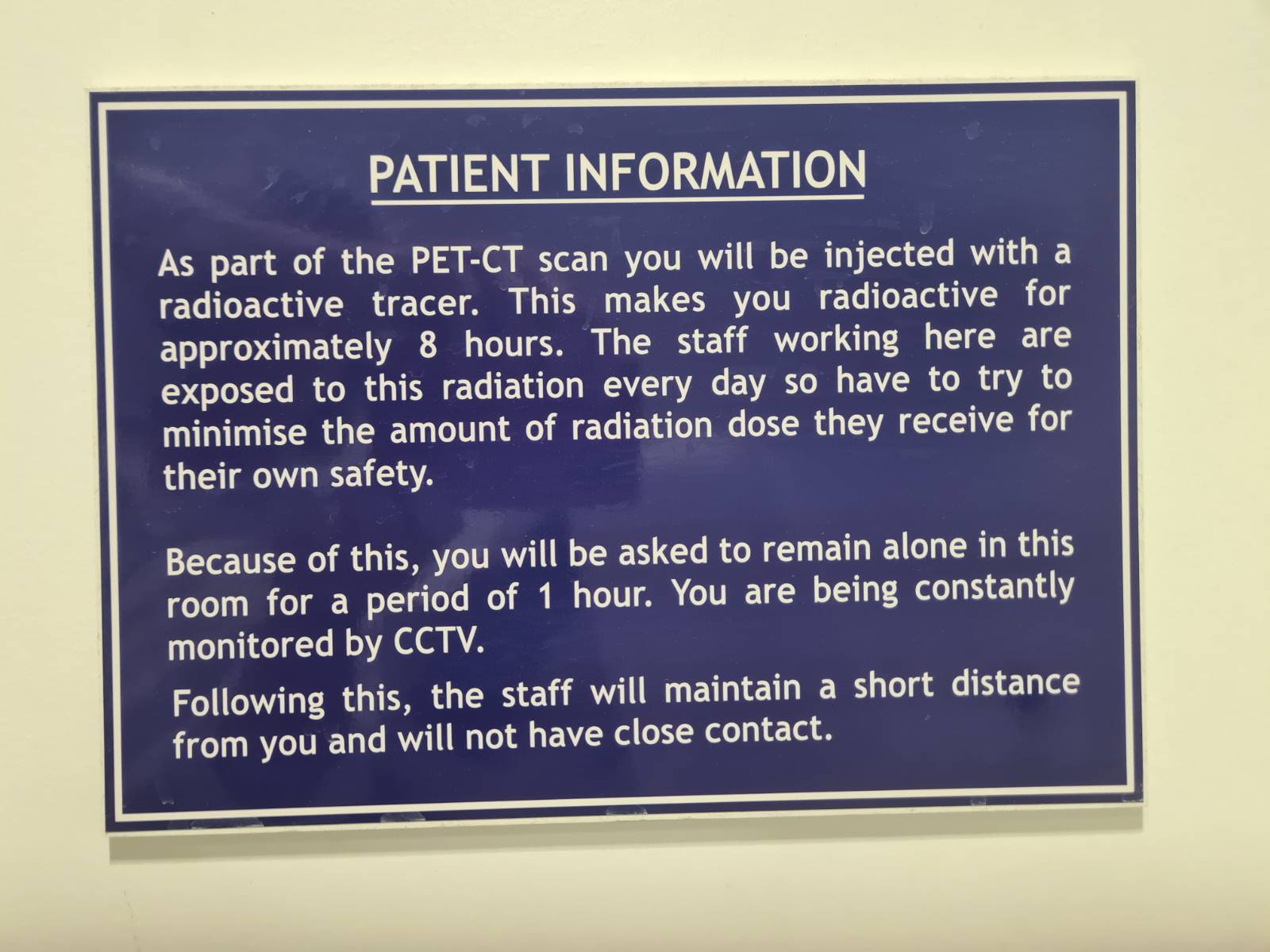
The doom vibes didn’t stop there. On arrival I was escorted to a little cell with radiation warnings on the door:

and I was gently and carefully injected with the radioactive tracer Gallium-68 and left sitting in this chair for quite a long time with the door shut:

Nobody wants to be invisibly poisoned with something so fierce it will leap inside other people and hurt them!
Just in case I didn’t get the message, there was a sign next to the chair:
But as experts and the UK government, and radiotherapy staff themselves often say, the general fear of medical radiation doesn’t make sense as applied to patients or their families. The sign is reasonable caution on behalf of staff who may potentially work in this environment for decades, but that isn’t the overall impression patients get. For myself as a member of the general public, I feel that if I am expected to adjust my behaviour because of invisible viruses, then I can be entrusted with accurate knowledge of radiation.
What to do?
For myself, I’m glad to have had one scan I thought I would not, and hopefully that’s the end of it.
The radiophobia starts long before the doctor or nurse says ’no’. The worrying misinformation trains people to just nod along, and can take the form of incorrectly telling parents a life-saving scan might cause their child to get cancer in years to come. So you should ask questions, including what harm has ever been observed. We already know the answer from the resources below and many similar ones: no clinical harm below a dose of roughly 14 PET scans delivered at once ↗ has been seen, and taking into account all evidence the risk for an individual patient is very small. Similarly for CT scans and other X-rays, the evidence is that the risk of the scan is lower than the risk of leaving the patient’s condition undiagnosed, including for children.
It also seems doctors who are not radiologists (and patients do not usually get to talk to radiologists) often don’t know much about radiation. Here in Scotland, a 2024 study across 4 health districts ↗ found that only 17% of doctors and medical students could score more than 50% on knowledge about medical radiation. In England a study found most clinicians overestimate radiation risks ↗ , with serious implications on patients, and may be applied throughout the UK.
Aberdeen is just fine
A strong piece of evidence is that people in Aberdeen do not show signs of increased cancer, even though the geology of the city gives off radioactivity equivalent to a PET scan every few years ↗ . And generations of people have lived in regions of Iran, China, India and Brazil with up to 30 times the radiation exposure most of us receive, but detailed studies have not shown increased cancer in these either.
This is about asking the right question.
Radioactivity can surely be dangerous, and 100 years ago its discoverer, Marie Curie, died from repeated unshielded medical X-ray exposure ↗ . Nothing like this extreme would ever be considered for a medical worker today. In addition she spent decades handling radioactive radium on a daily basis to the extent that her handprints on furniture are still visible to radiation monitors, but there was no finding that this radiation caused her death. Therefore a good question to ask is: What is a non-extreme dose of radiation? How much causes harm? Unfortunately, this question is not asked and for a very strange reason.
The reason this question is not asked starts with Hermann Muller’s 1946 Nobel Prize lecture ↗ , in which he described giving fruit flies very high doses of radiation (they didn’t like it) and then claimed any dose at all of radiation causes genetic damage. That was a nice neat statement anyone can understand. Ever since, when it comes to radioactivity safety, the following simplistic question is asked instead: Given that any dose causes harm, how much harm does this particular dose cause?
Many science papers have since shed light on this question, proposing instead that a much bigger risk is misdiagnoses due to phobia-driven lack of scans ↗ . Here in the UK, legislation caps occupational radiation workers at the equivalent of 3 PET scans per year ↗ , despite there being no evidence of harm to millions of people who live with 4x that amount all their lives from natural radiation. The UK legislation relies in part on a disputed US technical report called BEIR VII ↗ claiming a 1-in-136 lifetime risk of cancer for a nuclear radiation worker receiving less than half the annual dose of an Aberdonian. Unfortunately the way this number is applied is convenient for regulations protecting radiation workers, but it is not relevant to patients deciding whether to have their next scan.
Radiophobia directly causes other harms, including:
- Scan substitution, where children are fearfully diverted from CT scans, which use X-rays, to MRIs which do not, causing sedation risk to vulnerable children ↗ . The UK government places no upper limit on CT scans per year ↗ .
- many thousands of fear-driven elective abortions ↗ across Europe ↗ following the 1986 Chernobyl nuclear accident in Ukraine ↗ .
- 2300 deaths in the 2011 Fukushima nuclear accident in Japan ↗ , from fear-driven forcible relocation of communities and shutting down farms. No deaths or injuries were recorded due to radiation at Fukushima.
Cells cope because damage is normal
Each of the trillions of cells in our bodies suffers many thousands of DNA damage events every day ↗ caused by the business of being alive, and we have continuous molecular repair systems to deal with this. A PET scan delivers approximately 7 millisieverts of radiation, where a millisievert (mSv) is the unit for how much radiation the human body absorbs, from cosmic rays zipping through us, and radiated out of rocks, food, and the air. Given I live in Scotland but not in Aberdeen, I receive about 2.7 mSv per year from my surroundings. At 7 mSv, the additional DNA damage from the PET scan amounts to roughly one extra DNA break per four cells ↗ , which is far too low to measure or worry about.
There is an obvious objection: the scan happens in few hours, and if I had my annual dose of say, salt, in a few hours I would die! The answer is about capacity. My kidneys don’t have the capacity to clear that much salt in one go and so they choke, but our DNA repair capacity doesn’t start to get overloaded until at least hundreds of mSv, and nowhere near 7 mSv.
Summary
Further reading
The technical issue behind this article is the Linear No-Threshold (LNT) model, which is the statistical version of Muller’s Nobel Prize lecture. LNT draws a straight line of harm from atomic bomb survivor observations all the way down to zero, and many authorities including in the UK are reviewing it while simultaneously enforcing it. LNT is extremely attractive administratively because it is so simple. For a patient concerned about receiving a scan or not, starting points for further investigation include:
- Article in the journal “Dose-Response” on Radiophobia ↗ describing the “fabrication of health risks”, 2018.
- Background radiation and cancer incidence in Kerala, India — Karunagappally cohort study ↗ covers lack of cancer in around 400,000 residents, in 2009.
- In the UK, the 2025 Statement on Low Doses of Ionising Radiation ↗ acknowledges “risks at low doses are uncertain and estimates may change,” and reviews the situation described in this article. UK Safety Advice ↗ acknowledges the facts, although still not discussing how “all doses are harmful” may impact workers as distinct from patients, it does say that there is no upper limit on the number of CT scans that can be had in a year.
- Reevaluation of Radiation Protection Standards for Workers and the Public Based on Current Scientific Evidence ↗ is a 2025 US report that proposes eliminating all restrictions on low doses with unmeasurable effects, saying the no-dose-is-safe approach has morphed “from a philosophical aspiration into a binding legal requirement.”
Deeper analysis
If you are interested in scientific analysis, this isn’t an open-and-shut problem in general. It is only open-and-shut if someone needs a medical scan, in which case the answer is “yes, do it”, never “they may get cancer decades from now so do not”. The latter is radiophobia. Scientifically the larger picture is nuanced:
… as to the sign in the preparation room above: it is correct regarding staff. A PET-CT technologist receives roughly 1–5 mSv per year just from patient proximity (Alnaaimi 2017, Eakins 2022), with higher doses their hands. In a thirty-year career, that approaches dose levels where epidemiology has detected dose-response (Grant 2017, INWORKS / Leuraud 2015). The sign accurately applies the inverse-square-law and ALARA principles that keep cumulative staff dose below the 20 mSv/year occupational limit.
… as to childhood CTs: the absolute risk to any individual child from a clinically-indicated CT is so small that refusing the scan is likely the larger harm. The most recent large cohort study (Hauptmann et al. 2023) finds a measurable dose-response for paediatric brain cancer; even if this is multiply replicated, the absolute risk per scan for a typical brain CT remains in the range of a few cases per 10,000 which supports the radiophobia thesis. The published authors' own conclusion is to do the scans but optimise the dose, not to refuse them.
… as to LNT validity: this is very much under scrutiny in 2026, but regardless, the advice for individual patients offered a scan doesn’t change (just take the scan.) Recent data supports LNT in some aspects: the NCI 2020 monograph ↗ (Hauptmann et al., a meta-analysis of 26 low-dose studies) concluded that “new epidemiological studies directly support excess cancer risks from low-dose ionizing radiation”; the NCRP Commentary 27 review ↗ (Shore et al. 2019, Health Physics) concluded that “the preponderance of recent epidemiologic data on solid cancer is supportive of the continued use of the linear no-threshold model”; and the French nuclear-safety institute IRSN, whose former chair Maurice Tubiana led the most influential LNT-critical paper of 2009, has now published an institutional review ↗ (Laurier et al. 2023) concluding that “no other dose-risk relationship seems more appropriate for radiological protection purposes”. This support relates to the population-and-worker-protection purposes LNT was designed for.
… as to high-background-radiation regions: It is true that Aberdeen, Cornwall, parts of Iran, China, India and Brazil show no excess cancer despite high natural background. These studies do have confounding limits (migration, age structure, and statistical power.) The Kerala/Karunagappally finding can be viewed as evidence that chronic low-dose-rate exposure may be biologically different from acute exposure of the same total dose (Laurier 2023). This is a population/worker observation and does not change the “take the scan” advice to an individual patient.
… as to Marie Curie: The 1995 OPRI exhumation of her body concluded that Curie’s aplastic anaemia was primarily caused by her unshielded WWI X-ray work in Joliot-Curie’s “petites Curies” mobile units rather than the radium she handled daily for years. The kind of radiation that killed Curie is what the inverse-square law regulations exist to prevent in workers.
References
References for the Deeper Analysis section above.
Low-dose epidemiology
- Hauptmann M, Daniels RD, Cardis E, et al. “Epidemiological Studies of Low-Dose Ionizing Radiation and Cancer: Summary Bias Assessment and Meta-Analysis.” J Natl Cancer Inst Monogr 2020;2020(56):188–200. PMC8454205 ↗ . Meta-analysis of 26 studies with mean cumulative doses below 100 mGy.
- Hauptmann M, Byrnes G, Cardis E, et al. “Brain cancer after radiation exposure from CT examinations of children and young adults: results from the EPI-CT cohort study.” Lancet Oncol 2023;24(1):45–53. PMID 36493793 ↗ . 658,752-person multinational cohort; significant linear dose-response for paediatric brain cancer.
- Grant EJ, Brenner A, Sugiyama H, et al. “Solid Cancer Incidence among the Life Span Study of Atomic Bomb Survivors: 1958–2009.” Radiat Res 2017;187(5):513–537. PMID 28319463 ↗ . Significant solid cancer dose-response in the 0–100 mGy range; threshold estimate compatible with zero.
- Leuraud K, Richardson DB, Cardis E, et al. “Ionising radiation and risk of death from leukaemia and lymphoma in radiation-monitored workers (INWORKS): an international cohort study.” Lancet Haematol 2015;2(7):e276–e281. PMID 26436129 ↗ . 308,297 nuclear workers in three countries; significant leukaemia dose-response with no deviation from linearity.
Reviews defending the LNT model
- Shore RE, Beck HL, Boice JD Jr, et al. “Recent Epidemiologic Studies and the Linear No-Threshold Model For Radiation Protection — Considerations Regarding NCRP Commentary 27.” Health Phys 2019;116(2):235–246. PMID 30585971 ↗ .
- Laurier D, Billarand Y, Klokov D, Leuraud K. “The scientific basis for the use of the linear no-threshold (LNT) model at low doses and dose rates in radiological protection.” J Radiol Prot 2023;43(2):024003. doi:10.1088/1361-6498/acdfd7 ↗ . IRSN (France) institutional position. Open access.
Literature critical of the LNT
- Tubiana M, Feinendegen LE, Yang C, Kaminski JM. “The Linear No-Threshold Relationship Is Inconsistent with Radiation Biologic and Experimental Data.” Radiology 2009;251(1):13–22. PMC2663584 ↗ .
- Calabrese EJ, O’Connor MK. “Estimating risk of low radiation doses — a critical review of the BEIR VII report and its use of the linear no-threshold (LNT) hypothesis.” Radiat Res 2014;182(5):463–474. PMID 25325819 ↗ .
- Siegel JA, Pennington CW, Sacks B. “Subjecting Radiologic Imaging to the Linear No-Threshold Hypothesis: A Non Sequitur of Non-Trivial Proportion.” J Nucl Med 2017;58(1):1–6. The “fabrication of health risks” article in Dose-Response already cited inline (PMC6043928 ↗ ) sits in this same tradition.
Occupational dose to PET-CT staff
- Alnaaimi M, Alkhorayef M, Omar M, et al. “Occupational radiation exposure in nuclear medicine department in Kuwait.” Radiat Phys Chem 2017;140:233–237. Annual average effective dose ~4.5 mSv for technologists in a 7000-patient/year department.
- Eakins J, Hager L, O’Connor U, et al. “Personal dosimetry for positron emitters, and occupational exposures from clinical use of gallium-68.” J Radiol Prot 2022;42(3):031502. PMID 35947972 ↗ . UK Health Security Agency study specifically on Ga-68 (the tracer used in this article’s PET scan).
Fukushima evacuation-vs-radiation deaths
- Tanigawa K, Hosoi Y, Hirohashi N, Iwasaki Y, Kamiya K. “Loss of life after evacuation: lessons learned from the Fukushima accident.” Lancet 2012;379(9819):889–891.
- Murakami M, Ono K, Tsubokura M, et al. “Was the risk from nursing-home evacuation after the Fukushima accident higher than the radiation risk?” PLoS One 2015;10(9):e0137906.
- Hasegawa A, Ohira T, Maeda M, Yasumura S, Tanigawa K. “Emergency Responses and Health Consequences after the Fukushima Accident; Evacuation and Relocation.” Clin Oncol (R Coll Radiol) 2016;28(4):237–244.
Marie Curie cause of death
- Office de Protection contre les Rayonnements Ionisants (OPRI), 1995 exhumation findings, summarised in: Abergel R, Aris J, Bolch WE, Dewji SA, et al. “The enduring legacy of Marie Curie: impacts of radium in 21st century radiological and medical sciences.” Int J Radiat Biol 2022;98(4):764–774. Concludes Curie’s aplastic anaemia was most likely caused by external X-ray exposure during her WWI radiology field work, not by lethal radium intake.